


- Posted on 10 Apr 2026
- 2-minute read
A computational study shows for the first time how different parts of the human airway experience levels of pressure and friction from breathing therapy devices.
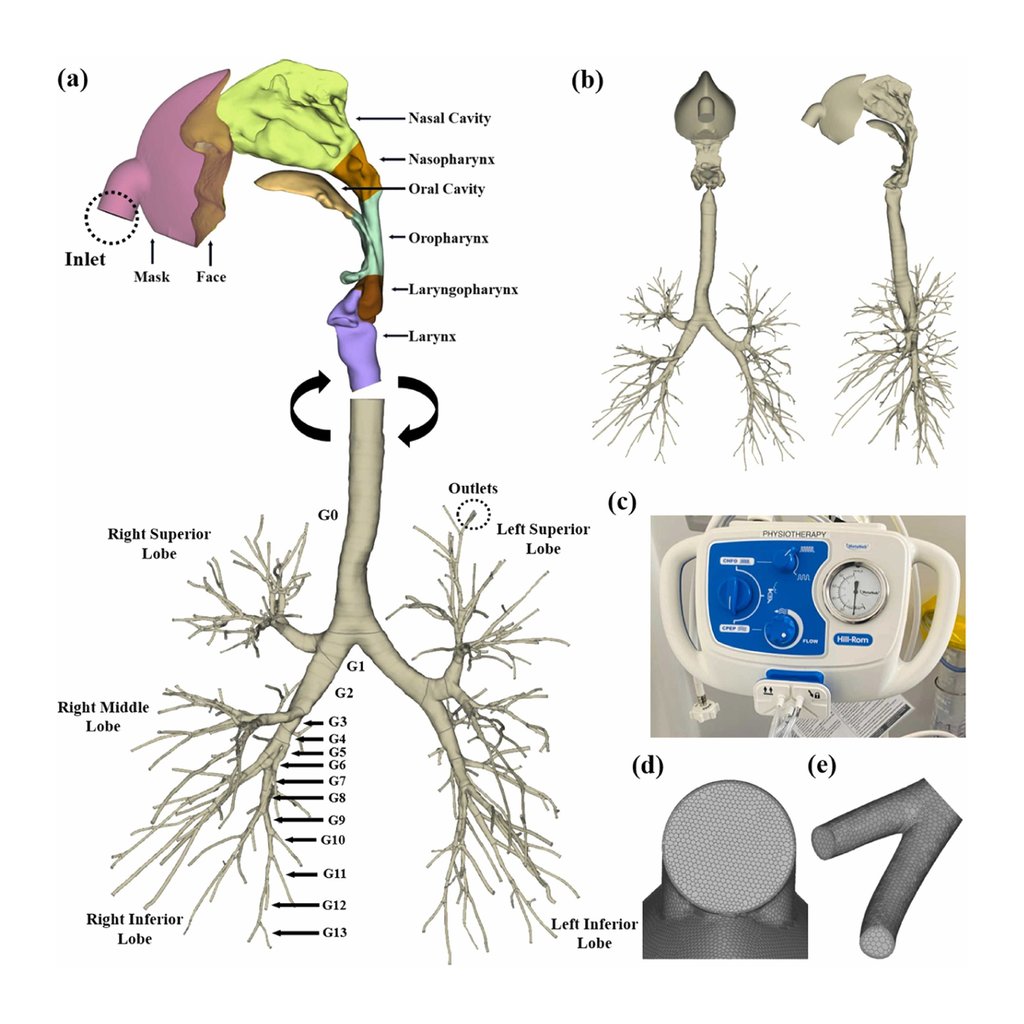
Using a patient-specific 3D airway model derived from CT imaging to simulate how breathing-support therapy behaves inside the human airway, University of Technology Sydney (UTS) researchers found the therapy doesn’t affect all parts of the airway equally.
The study shows the potential to support the design of better devices and personalised treatment settings for patients with conditions such as bronchiectasis, cystic fibrosis and postoperative atelectasis.
The paper, titled Modeling and simulation of conducting airways during continuous high-frequency oscillation therapy, was recently published in Respiratory Physiology & Neurobiology, Elsevier.
Lead author Dr Suvash C. Saha, Senior Lecturer in the UTS School of Mechanical and Mechatronic Engineering, said the study gives one of the clearest pictures yet of how breathing therapy moves through the human airway.
“Continuous high-frequency oscillation therapy (CHFO) is used clinically to support airway clearance and lung expansion, yet the way its oscillatory pressure is transmitted through the human conducting airways has remained poorly measured,” said Dr Saha.
“Our study helps fill that gap by mapping how CHFO reshapes pressure, wall shear stress and wall-normal loading throughout the conducting airway tree under both standard and high-pressure settings.”

“A computer model based on real human anatomy can reveal things that are very difficult to measure directly in patients, helping doctors and researchers make more informed decisions.”
The findings show that different parts of the airway, especially around the throat and upper airway, experience different levels of pressure and friction, so device settings may need to be chosen more carefully for different patients and clinical goals.
“We found that some areas, especially around the throat and voice box, experience much stronger pressure and friction than others, while larger upper-airway regions carry more of the overall force,” said Dr Saha.
“Turning the therapy up to a higher-pressure setting increases the strength of the support, but it does not change where the main effects happen.
“The airway anatomy itself plays a dominant role in fixing where mechanical loading is concentrated. Even when the therapy setting changes, those key anatomical hot spots remain,” said Dr Saha.
“We need a greater understanding of where and how the therapy acts to help improve safety, comfort and effectiveness in the future. It can eventually support the design of better devices and treatment settings.”
Dr Saha believes using advanced engineering and medical research together has the potential to improve healthcare such as CHFO.
“A computer model based on real human anatomy can reveal things that are very difficult to measure directly in patients, helping doctors and researchers make more informed decisions,” he said.
“This work supports the need for more evidence-based design and testing of respiratory support devices, including patient-specific modelling where possible.
“It also points to the value of future clinical guidelines that consider not just whether a therapy is used, but how different settings may affect different parts of the airway.”
Researchers:
Dr Suvash C. Saha, Senior Lecturer, School of Mechanical and Mechatronic Engineering, University of Technology Sydney
Mr Xinlei Huang, Researcher / first author, School of Mechanical and Mechatronic Engineering, University of Technology Sydney
Dr Isabella Francis
Professor YuanTong Gu, School of Mechanical, Medical and Process Engineering, Queensland University of Technology
News by topic

News
Bradfield City biosolar roof sets new standard for climate-resilient cities
A study of Bradfield City’s First Building green roof confirms that combining native rooftop gardens with solar panels reduces urban heat, increases renewable...

News
Friday essay: is there a great Australian graphic novel?
Comic-art makers and avid readers agree: if the great Australian graphic novel exists, what makes it great just might surprise you.

News
Educating for a changing world
New UTS Institute for Education prepares future teachers and education leaders.

News
Mind-reading AI pioneer wins global award
World-leading AI researcher Distinguished Professor CT Lin honoured with international Lofti A Zadeh Award for advancing technology to better connect the human...
News
Bradfield City biosolar roof sets new standard for climate-resilient cities
A study of Bradfield City’s First Building green roof confirms that combining native rooftop gardens with solar panels reduces urban heat, increases renewable...
News
Friday essay: is there a great Australian graphic novel?
Comic-art makers and avid readers agree: if the great Australian graphic novel exists, what makes it great just might surprise you.
News
Educating for a changing world
New UTS Institute for Education prepares future teachers and education leaders.
News
Mind-reading AI pioneer wins global award
World-leading AI researcher Distinguished Professor CT Lin honoured with international Lofti A Zadeh Award for advancing technology to better connect the human...